Barlow’s Mitral Valve Surgery: When is the Right Time?
Written By: Allison DeMajistre, BSN, RN, CCRN
Medical Expert: Marc Gerdisch, MD, Chief of Cardiac Surgery, Franciscan Health, Indianapolis, Indiana
Reviewed By: Adam Pick, Patient Advocate, Author & Website Founder
Published: August 14, 2025
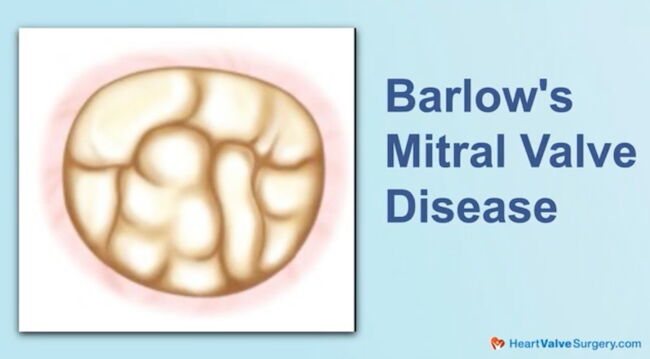
Many people live their entire lifetime with mitral valve prolapse without any symptoms or need for an intervention. However, patients diagnosed with Barlow’s mitral valve disease often have a much different experience with this type of mitral valve prolapse because of its degenerative nature. Many patients live with Barlow’s mitral valve from childhood with no symptoms or complications.
Over time, though, the mitral valve leaflets can become thickened, the mitral annulus dilates, and the chordae tendineae, also known as “heart strings,” that connect the valve leaflets to the papillary muscle, start to stretch, increasing prolapse and the back-flow of blood into the left ventricle and right atrium. Eventually, some type of intervention is warranted to either repair or replace a weakened Barlow’s mitral valve, even if patients do not exhibit any of the typical symptoms associated with mitral regurgitation, such as shortness of breath, dizziness, or rapid heartbeat. Understanding the timing and type of surgery is imperative to prevent complications like heart failure, abnormal heart rhythms, stroke, and even sudden cardiac death.
We just received a great patient question on this topic from Amy, who has a Barlow’s valve. Amy asked, “I’m a 47-year-old female with known mitral valve prolapse from a Barlow’s valve since I was a child. Regurgitation is now moderate to severe with multiple jets, and tricuspid regurgitation is mild to moderate. My atrium is mildly dilated. Should valves be repaired while heart function is still normal, and if so, what is the likelihood of getting both mitral and tricuspid valves repaired, not replaced?” To answer Amy’s question, we met with Dr. Marc Gerdisch, the Chief of Cardiac Surgery at Franciscan Health in Indianapolis, Indiana. Dr. Gerdisch has successfully treated over 100 patients in the HeartValveSurgery.com community and is always a phenomenal resource for obtaining answers about complex forms of heart valve disease and surgery.
Understanding When to Treat Barlow’s Mitral Valve
Here are the key insights shared by Dr. Gerdisch:
- Asymptomatic patients often do not know the extent of their disease. “It’s a very insightful question,” said Dr. Gerdisch. “It’s true that a lot of folks with valve problems, mitral regurgitation specifically, who are otherwise healthy, don’t become symptomatic and aren’t aware that they have the problem, which can cause us to lose ground with those ventricles. The reason for this is that the ventricle becomes volume overloaded and, over time, starts to change shape, potentially not returning to normal. Specifically, in a Barlow valve with multiple jets, when we perform a transesophageal echocardiogram and study it thoroughly, we often find that it’s severe.
- How to assess the extent of the disease. “Because there are multiple jets, they need to be summated to determine the regression volume,” explained Dr. Gerdisch. “The left atrium being enlarged is a little bit of an indicator. We’d like to get actual dimensions and a better look at it, but I am concerned that the tricuspid valve is leaking. So, moderate tricuspid insufficiency needs to be addressed; it can’t be left alone. But it’s also an indicator that perhaps the process has moved along a bit. Now, people can have myxomatous changes. They can also have changes in their tricuspid valve that are also organic, but usually it’s secondary to the mitral regurgitation, so we would want to ascertain whether that was the case.”
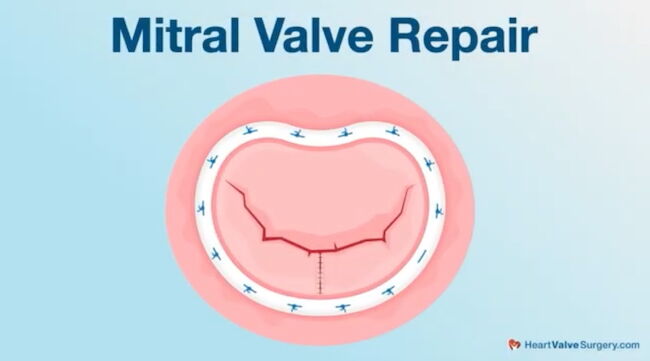
- Should the valve be repaired or replaced? “Both valves would be repaired,” said Dr. Gerdisch. “For surgeons who do a lot of mitral valve repair, the likelihood that the valves will be repaired is almost 100 percent. It’s important that Amy work with people who are comfortable with some certainty about the repair method for the mitral valve, whether that involves minimally invasive surgery, which is our preferred approach, or a sternotomy. Either way, the most important thing is that the valves be preserved.”
Thanks Dr. Gerdisch and Franciscan Health!
On behalf of all the patients in our community, thank you, Dr. Marc Gerdisch, for everything you and your team are doing at Franciscan Health in Indianapolis, Indiana!
Related links:
- See 125+ Patient Reviews for Dr. Marc Gerdisch
- Free Heart Valve eBook: Ask Dr. Gerdisch Anything
- Surgeon Q&A: Minimally-Invasive Mitral Valve Surgery
- Rapid Recovery Protocol 2.0: What Should You Know?
Keep on tickin,
Adam
P.S. For the deaf and hard-of-hearing members of our patient community, we have provided a written transcript of our interview with Dr. Gerdisch below.
Written by Adam Pick
- Patient & Website Founder

Video Transcript:
Adam Pick: Hi everybody, it’s Adam with HeartValveSurgery.com and we’re in Los Angeles, California at the Society of Thoracic Surgeons Conference. I am thrilled to be joined by Dr. Mark Gerdisch, who is the Chief of Cardiac Surgery at Franciscan Health in Indianapolis, Indiana.
Dr. Gerdisch, we have known each other for over 10 years. You’ve successfully treated over a hundred patients in our community. We’re here at STS and it’s always a gift to be in your presence. Thanks for being with me today.
Dr. Mark Gerdisch Thanks. Always a pleasure.
Adam Pick: We’re going to answer a patient question that came in today from Amy and Amy asks, “I’m a 47 year old female with known mitral valve prolapse from a Barlow’s valve since I was a child. Regurgitation is now moderate to severe with multiple jets and tricuspid regurgitation is mild to moderate. My atrium is mildly dilated. Should valves be repaired while heart function is still normal, and if so, what is the likelihood of getting both mitral and tricuspid valves repaired, not replaced?”
Dr. Mark Gerdisch: Right, so it’s a very insightful question. And it’s actually true that a lot of folks with valve problems, mitral regurgitation specifically, who are otherwise healthy, they don’t become symptomatic, so Folks aren’t aware that they have the problem and we can lose ground with those ventricles. And the reason for that is the ventricle becomes volume overloaded and over time starts to change shape and it may not go back to normal.
So, specifically to a Barlow with multiple jets, often when we do a transesophageal echocardiogram and study it well, we find that it’s actually severe. Because there’s multiple jets, they need to be summated to determine the regression volume. The left atrium being enlarged is a little bit of an indicator, we’d like to get actual dimensions on that and get a better look at it, but I am concerned that the tricuspid valve is leaking.
So, moderate tricuspid insufficiency needs to be addressed, it can’t be left alone. But it’s also an indicator that perhaps the process has moved along a bit. Now people can have myxomatous changes, they can have changes in their tricuspid valve too that are organic, but usually it’s secondary to the mitral regurgitation, so we would want to ascertain whether that was the case.
The answer to the repair question is that yes, they would both be repaired. Uh, for folks who do a lot, surgeons who do a lot of mitral valve repair, it’s almost 100 percent likelihood that that valve will be repaired. So it’s important that she work with people that are going to be comfortable with some certainty to repair the mitral valve, whether that’s minimally invasive the way we would do it or through a sternotomy. Either way, the most important thing is that the valves be preserved.
Adam Pick: Amy, I hope that helped you. I know it helped me and Dr. Gerdisch on behalf of all the patients, all over the world, thanks for everything you and your team are doing at Franciscan Health. In Indianapolis, Indiana. Thanks so much for being with me today.
Dr. Mark Gerdisch: Thanks, Adam.




