The Ross Procedure: What Should Patients Know?
Written By: Allison DeMajistre, BSN, RN, CCRN
Medical Expert: Vaughn Starnes, MD, Surgeon-in-Chief, Keck Medicine of USC, Los Angeles, California
Reviewed By: Adam Pick, Patient Advocate, Author & Website Founder
Published: June 18, 2025
The Ross Procedure offers patients with severe aortic stenosis and aortic regurgitation a renewed chance to live a longer, better quality of life. As many of our community members know, Adam Pick, the founder of HeartValveSurgery.com had a Ross Procedure nearly two decades ago. This unique “two-valve” procedure provided Adam a normal life without any reoperation and without the use of blood thinners.
In this very special interview, Adam speaks with Dr. Vaughn Starnes, the surgeon who performed his Ross Procedure. Dr. Starnes, the Surgeon-in-Chief of Keck Medicine of USC in Los Angeles, California, has performed over 650 Ross Procedures during the past 30 years. We were very excited to learn more about this complex yet life-changing operation.
About The Ross Procedure
Here are the questions Adam asked and the key insights shared by Dr. Starnes:
- How many Ross Procedures have you performed, and why did you bring it into your practice? “I’ve been in practice with the Ross Procedure since 1992 when I moved to Los Angeles from Stanford,” said Dr. Starnes. “I brought it into my practice because I just felt like the Ross gave patients back an exceptional quality of life. They didn’t have to be on a blood thinner. After recuperation and a period of four to five months, they could return to doing anything they wanted to do. I embraced that, and I’ve been doing Ross operations ever since. My practice now is a little over 650 Ross Procedures that I’ve completed. It’s really been rewarding to follow these patients long-term, and I have some patients out 30 or 32 years now.”
 The Ross Procedure
The Ross Procedure
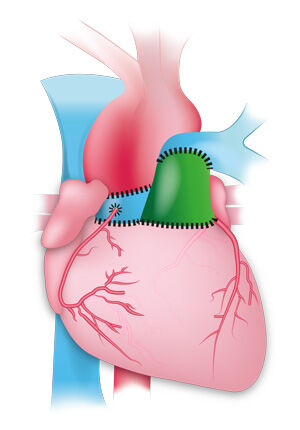
- Many patients in our community are not aware of the Ross Procedure. Can you explain what it is? “Well, Donald Ross came up with this operation in 1967,” Dr. Starnes explained. “During the Ross Procedure, we put the patient on the heart lung machine. Then, we stop the heart, open up the aorta, remove the aortic valve, remove the pulmonary valve, and move it into the aortic position. Then, we re-establish the pulmonary valve, usually with either a human or maybe a porcine or pericardial valve.”
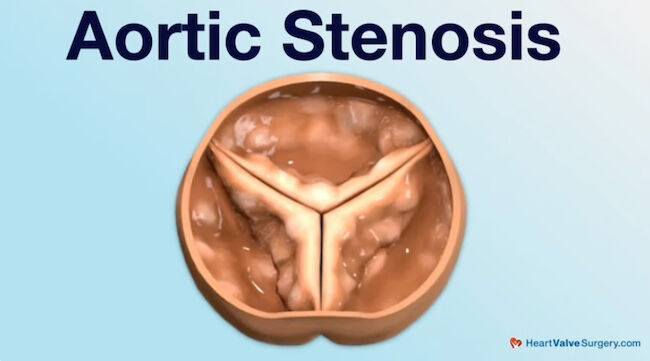
- What types of aortic valve disease does the Ross Procedure treat? “It’s evolved over time as we’ve gained more and more experience,” said Dr. Starnes. “Right now, I would say patients with aortic stenosis primarily are candidates for the Ross Procedure. Those are patients with calcified valves. A lot of patients have bicuspid aortic valves. We used to think patients with dilated aortic annulus or regurgitation were not great candidates. But now, with our inclusion technique, we also take on those patients. So, now it is a valve replacement for all types of aortic valve disease.”
- Is the Ross Procedure more complex than other surgical aortic valve replacement forms that might include a mechanical or bioprosthetic valve? “Yes, it’s very different. In a standard mechanical or pig valve replacement, you remove the leaflets, do nothing to the root, and don’t take out the coronaries. You simply take out the diseased valve, insert a prosthetic valve in its place, and sew it in the annulus,” he explained. “There are 15 or 16 interrupted sutures. You put the valve in and close the aorta. It’s pretty straightforward. With the Ross Procedure, you actually do a root replacement. You take out the valve and remove the coronaries, then move over to the right side and take out the pulmonary valve. You transect it at the level of where the pulmonary bifurcates, and then you make an incision in the right ventricular outflow tract. Then you, as I say, innuculate that valve from the right ventricle, and in doing so, you’ve got to avoid the left coronary artery and the septal perforator. Then, you move the pulmonary valve over and sew that in the aortic annulus like a standard valve and re-implant the coronaries. And then you go back over to the right side and reconstruct the right ventricular alpha tract. So, it’s a very complicated operation.”
- Can the Ross Procedure be done minimally invasively? “No, it’s a standard open sternum operation because you must have good exposure to the pulmonary and the aortic sides. So, no minimally invasive approach to this is safe.”
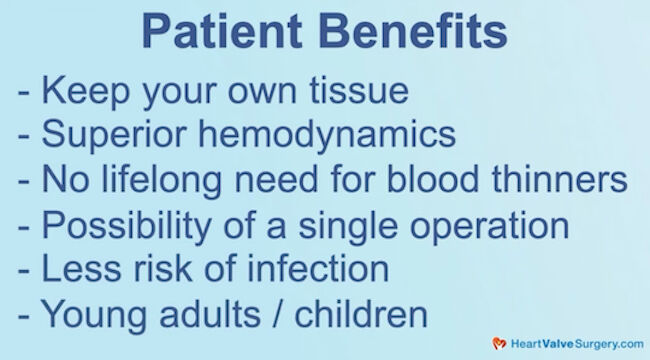
- What are the patient advantages of the Ross Procedure? Dr. Starnes said, “You keep your own tissue so it can repair itself. It has superior hemodynamics, no need for lifelong blood thinners, and the possibility of just having a single operation. There is less risk of infection, and in young adults and particularly children, there is the potential for growth.”
- What is the latest research on the survivorship and durability of the Ross? “Great question,” said Dr. Starnes. “After doing it for 30 years, you learn things you can improve upon. One of the great things we’ve found now by following these patients is that survivorship equals that of the general population. If a patient 10 years ago had a mechanical valve or even a pig valve, after 15 or 20 years, 15 to 20 percent of them have died. That’s not the case with the Ross Procedure. They have survival benefits that equal the general population. The other thing we’ve discovered is that the autograft can dilate and become leaky with the Ross. So now, we support it at the annular level or by doing a total inclusion. That’s almost eliminated the failure point of the Ross, which is dilation and regurgitation.”
- What have been your patient outcomes with the Ross Procedure? “Mortality rates are close to zero,” he said. “I don’t think we’ve lost a patient in the last 10 years, and we’re very proud of that. We also have failure rates down to about three percent.”
- What is your number one piece of advice for someone considering the Ross Procedure? Dr. Starnes said, “Number one, when in your local medical center, you need to ask, ‘Who’s doing the Ross Procedure in my city? How many have they done and what is their outcome?’ It is all important data that you should have on hand before you make a decision. The Ross is something worth traveling for. It’s a great operation with great outcomes. It gives you the potential to have a normal life, so I believe you should travel if it’s not available in your local city or town.”
Thanks Dr. Starnes and Keck Medicine of USC!
On behalf of all the patients in our HeartValveSurgery.com community, thank you to Dr. Vaughn Starnes for everything you and your team are doing at Keck Medicine of USC in Los Angeles, California!
Related links:
- See 100+ Patient Reviews for Dr. Vaughn Starnes
- Discover the new Ross Procedure Patient Education Center
- Dr. Vaughn Starnes Named the 100th President of AATS
P.S. For the deaf and hard-of-hearing members of our patient community, we have provided a written transcript of our interview with Dr. Starnes below.
Written by Adam Pick
- Patient & Website Founder

Video Transcript:
Adam Pick: Hi everybody, it’s Adam with HeartValveSurgery.com. We’re in Los Angeles, California at the Society of Thoracic Surgeons Conference. I’m thrilled to be joined by Dr. Vaughn Starnes, who is the Surgeon in Chief of Keck Medicine of USC. Dr. Starnes, we’re here at STS talking about the Ross procedure. It is great to see you again.
Dr. Vaughn Starnes: Likewise.
Adam Pick: So everybody knows… Nearly two decades ago, this man performed a successful Ross procedure on me.
Since then I’ve gone on to get married. I’ve had a child. I have returned to all of the life activities that I love, including SCUBA diving and traveling the world. And so, I can’t think of anybody better to have this conversation with and learn about your 30-year experience with the Ross procedure.
So let’s start. Dr. Starnes, how many Ross procedures have you performed and why did you bring it into your practice?
Dr. Vaughn Starnes: Well, Adam, I have been in practice with the Ross Procedure since 1992 when I moved to Los Angeles from Stanford. I brought it into my practice because I just felt like the quality of life after you did a Ross that you gave back to the patients would be exceptional.
They didn’t have to be on a blood thinner. After a recuperation and after a period of four to five months, they could return to do anything they wanted to do. I embraced that. I’ve been doing Ross operations ever since. My practice now is a little over 650 Ross Procedures that I’ve completed. It’s really been rewarding to follow these patients long term, like yourself. And I have some patients out 30, 32 years now.
Adam Pick: Dr. Starnes, you have embraced this procedure and empowered patients, like myself, to have such a great life, so thank you for that. There are people in our community who may have never heard of the Ross procedure. Can you explain what it is?
Dr. Vaughn Starnes: Sure. Well, Donald Ross in 1967, came up with this operation. During the Ross procedure, we put the patient on the heart lung machine. Then, we stop the heart, open up the aorta, remove the aortic valve, and then we take out the pulmonary valve and move it over into the aortic position. Then we, re-establish the pulmonary valve, usually with either a human or maybe a porcine or pericardial valve.
Adam Pick: Fascinating. I’m curious to know what types of aortic valve disease does the Ross Procedure treat?
Dr. Vaughn Starnes: Yes, it’s, it’s evolved over time as we’ve gained more and more experience. Right now, I would say patients with aortic stenosis primarily are candidates for the Ross procedure. Those are patients with calcified valves.
A lot of patients have bicuspid aortic valves. We used to think that patients with dilated aortic annulus or regurgitation were not great candidates. But now, with our inclusion technique, we take on those patients also. So, it now really is a valve replacement for all types of aortic valve disease.
Adam Pick: Dr. Starnes, it’s great to hear how you are using the Ross procedure for different types of aortic valve patients. Is this procedure more complex than other forms of surgical aortic valve replacement that might include a mechanical or a bioprosthetic valve?
Dr. Vaughn Starnes: Yes, Adam. It’s very different. In a standard, say, a mechanical valve replacement or a pig valve replacement, you remove the leaflets, you do nothing to the root, you don’t take out the coronaries, you simply take out that disease valve and insert a prosthetic valve in place and sew it in in the annulus. You know, 15 or 16 interrupted sutures, put the valve in, move it in. Close up the aorta. Pretty straightforward.
With the Ross procedure, you actually do a root replacement. So, you take out the valve, you take off the coronaries, and then you move over to the right side, and you take out the pulmonary valve. So, you transect it at the level of where the pulmonary bifurcates, and then you make an incision in the right ventricular outflow tract.
And then you, as I say, innuculate that valve from the right ventricle. And in doing so, you’ve got to avoid the left coronary artery, you’ve got to avoid the septal perforator. So, it’s very much a complicated operation. And then you move the pulmonary valve over, and then you sew that in the aortic annulus like you would a standard valve, and then you re-implant the coronaries.
And then you go back over to the right side and reconstruct the right ventricular alpha tract,
Adam Pick: Dr. Starnes, Wow! This is very complex. I’m sure some patients are wondering, is this something that can be done minimally invasively?
No, it’s not. It’s a standard open sternum operation because you have to have good exposure both of the pulmonary side and the aortic side. So, there’s no minimally invasive approach to this that’s safe.
Dr. Starnes, what are the patient advantages of the Ross procedure?
Dr. Vaughn Starnes: The patient benefits of the Ross procedure… Number one, you keep your own tissue so it can repair itself. It’s got superior hemodynamics, no lifelong need for blood thinners, possibility of a single operation, less risk of infection, and in young adults, particularly children, the potential for growth.
Adam Pick: Dr. Starnes, those are a lot of great patient benefits. Can we dive deeper into the survivorship and the durability of the Ross? What’s the latest research coming out about the Ross surgery?
Dr. Vaughn Starnes: Great question, Adam. After you’ve been doing it for 30 years, you learn things about it you can improve upon. One of the great things that we’ve found now by following these patients is that survivorship equals that of the general population. If a patient 10 years ago had a mechanical valve or even a pig valve, unfortunately at 15, 20 years, 15 to 20 percent of them are no longer with us. They’ve died.
That’s not the case with Ross procedure. They have survival benefits that equal the general population. The other thing we’ve known, or we’ve discovered, is that with the Ross procedure, the autograft can dilate and it can become leaky. So now, we support it either at the annual level or even doing a total inclusion.
That’s really eliminated almost the failure point of the Ross procedure, which are dilation and regurgitation.
Adam Pick: Dr. Starnes, I love hearing about the innovations and the improvement of durability of the Ross Procedure. I’m curious to know, when it comes to the outcomes, can you share with the patients, what have been your outcomes for patients with the Ross operation?
Dr. Vaughn Starnes: Well, number one… Mortality rates is close to zero. I don’t think we’ve lost a patient in the last 10 years. So we’re very proud of that. Failure rates, we’ve got it down to about 3%.
Adam Pick: Dr. Starnes, these are fantastic outcomes. And I have to ask you on behalf of the patients in our community, what is your number one piece of advice for someone considering the Ross procedure?
Dr. Vaughn Starnes: Number one, when in your local medical center, local town, you need to ask the question, “Who’s doing the Ross procedure in my city?”
How many have they done? What is their outcome? I mean, all this is data that you should have on hand before you make a decision.
The Ross Procedure is something worth traveling for. It’s a great operation It’s great outcomes. It gives you the potential to have a normal life. So, I, I think traveling, if it’s not available in your local city or town, you should do it.
Adam Pick: Well, that is extraordinary advice for all the people watching this. And on behalf of the patients, at HeartValveSurgery.com, patients all over the world and, in particular, my family, thank you for giving me back an extraordinary life. I cannot thank you enough. It’s been great seeing you Dr. Starnes.
Dr. Vaughn Starnes: Always Adam, always.
Adam Pick: Thanks so much for your help.
Dr. Vaughn Starnes: Thank you.




