Innovation Update: Robotic Aortic Valve Replacement
Written By: Allison DeMajistre, BSN, RN, CCRN
Medical Expert: Vinay Badhwar, MD, Executive Chair of WVU Heart & Vascular Institute, Morgantown, West Virginia
Reviewed By: Adam Pick, Patient Advocate, Author & Website Founder
Published: November 8, 2025
Although surgeons have been performing robotic mitral valve repair and replacement for over twenty years, treatment for aortic valve disease has primarily been done with surgical aortic valve replacement (SAVR) via median sternotomy and, more recently, with transcatheter aortic valve replacement (TAVR) using a percutaneous approach. Over the last five years, however, robotic aortic valve replacement has begun to emerge as a viable option for patients as more surgeons from the United States and around the world have learned from one another and mastered the technique.
Dr. Vinay Badhwar, the Executive Chair of the WVU Heart & Vascular Institute in Morgantown, West Virginia, has been at the forefront of this surgical innovation and continues to collaborate with surgeons worldwide as the technology advances. Adam Pick, the founder of HeartValveSurgery.com, met with Dr. Badhwar at the Endoscopic Cardiac Surgeons Club Meeting in Northern Kentucky to learn more about this exciting new surgical technique for aortic valve replacement.
The Latest Developments in Robotic Aortic Valve Replacement
Here are the key insights shared by Dr. Badhwar:
- Patients in the community often ask about the latest updates regarding robotic aortic valve replacement (RAVR). “First of all, I am delighted that your patients and your colleagues are asking about robotic AVR,” said Dr. Badhwar. “Our goal was to develop another option for patients besides having a sternotomy, anterior chest approach, or a transcatheter valve. The robotic option gives the same outcome as a regular surgical aortic valve. It has lots of evidence for long-term survival, low morbidity, and fewer problems over the lifespan of the patient.”
- What has been achieved since the first surgical case? “We did our first case in January of 2020,” said Dr. Badhwar. “That was a collaboration, not just among our surgical team, but also our transcatheter cardiologists who wanted to have another option for the low to intermediate risk patients, particularly those who are younger than age 80. Since January 2020, after treating the first 200 patients, we’ve opened this up to the rest of the world. We’re very pleased to have a close collaboration with many of the surgeons here today and others around the world. There have now been nearly 400 patients who have received this therapy. After commencing this at WVU, there has been significant overall development, and the outcomes have been truly outstanding. Our key focus is to make this safe, standardized, and reproducible.”
- In terms of when you’re using the robot, is it isolated to a robotic AVR, or has its ability for other treatments widened over the years? “That’s a very important question,” said Dr. Badhwar.” “There are many options for treating patients with valvular heart disease. Transcatheter therapy is a single therapy, or a TAVR or TAVI, to treat the aortic valve. But many of our patients have other things like atrial fibrillation, mitral valve disease, et cetera. While we can do isolated robotic aortic valve replacement or repair, the whole reason we wanted to develop this through a tiny right lateral mini thoracotomy incision is to be able to use the same approach we use for standardized mitral valve surgery.” Dr. Badhwar explained that up to a third of the patients they treat don’t just need treatment for aortic valve disease. They also need treatment for mitral valve disease, atrial fibrillation, and other problems that go along with valvular disease. “We feel strongly that this is now a platform, not just for isolated aortic valve disease, but for all cardiac and multiple valvular surgeries.”
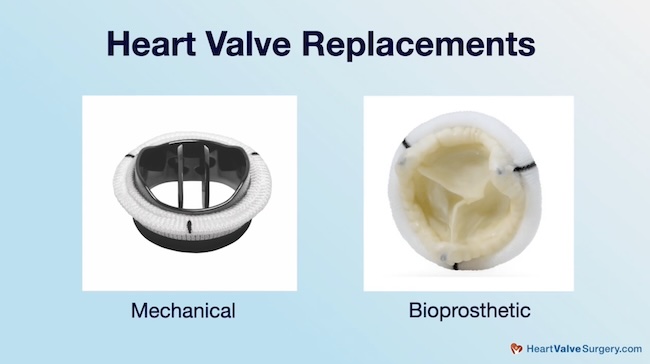
- Is the robotic AVR for a mechanical valve or for a tissue valve? “Using a very standardized surgical treatment, we cut out the valve and sew on a brand new one. It can either be a biologic valve made of cow or pig tissue, or a mechanical valve. There have been excellent outcomes for both,” explained Dr. Badhwar.
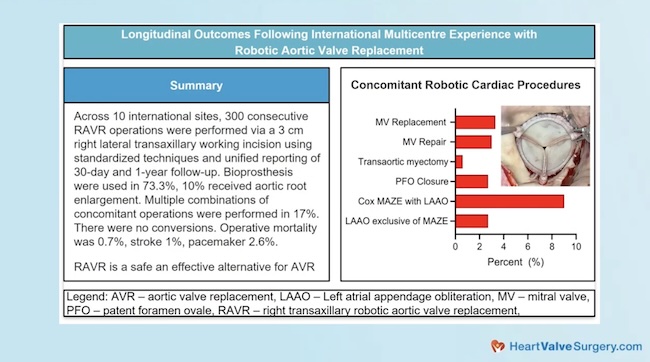
- What is the next step for sharing this information with physicians here and around the world? “We’ve worked this up in a very transparent way,” said Dr. Badhwar. “Innovation in isolation remains in isolation. Innovation as a collaboration becomes permanent. At least we hope. Starting in 2022, shortly after our initial experiences, we invited surgeons from around the world to co-develop and share their experiences. Last year, at the European Association for Cardiothoracic Surgery, we published our results for the first 300 patients. This was an international collaboration with multiple sites around the United States and Europe. Now, it has culminated in over 400 patients, and we are hosting another international valve meeting in Morgantown on November 13th and 14th. It’s called the International RAVRs Symposium, where surgeons and cardiologists will hopefully share ideas and their own experiences, and how to make this a better therapy for all our patients.”
Thanks Dr. Badhwar and WVU Heart and Valvular Institute!
On behalf of all the patients in our community, thank you, Dr. Vinay Badhwar, for everything you and your team are doing at the WVU Heart and Valvular Institute in Morgantown, West Virginia!
Related links:
- See Dr. Badhwar’s Interactive Surgeon Profile
- Badhwar: Top 3 Mitral Valve Repair Innovations
- Explore the WVU Heart and Vascular Institute Microsite
Keep on tickin,
Adam
P.S. For the deaf and hard-of-hearing members of our patient community, we have provided a written transcript of our interview with Dr. Badhwar below.
Written by Adam Pick
- Patient & Website Founder

Video Transcript:
Adam Pick: Hi everybody. It’s Adam with HeartValveSurgery.com, and we’re at the Endoscopic Cardiac Surgeons Club in Northern Kentucky. I am thrilled to be joined by Dr. Vinay Badhwar, who is the executive chair of the WVU Heart and Vascular Institute. Morgantown, West Virginia.
Dr. Badhwar, you and I have known each other for going on 15 years. Great to see you, and thanks for being with me today.
Dr. Vinay Badhwar: Glad to be here, Adam.
Adam Pick: So we are learning a ton here. Research, live operations, simulations, right in your sweet spot of minimally invasive surgery. I know you’re giving talks here. One of the big inquiries that we get from patients is about robotic aortic valve replacement, which is something if anybody in the world knows about, it’s you, can you share with the patients in our community, “What’s the latest update on robotic aortic valve replacement (RAVR)?
Dr. Vinay Badhwar: Well, first of all, I am delighted that your patients and the, and the colleagues that you have, are asking about robotic AVR. Given the fact that our whole goal was to develop another option. For patients instead of having a sternotomy or an anterior chest approach or a transcatheter valve, another option that gives the same outcome of a regular surgical aortic valve, which has lots of evidence for long-term survival and low morbidity and problems, uh, for the lifespan of the patient. And so we did our first case in January of 2020. That was a collaboration, not just amongst our surgical team, but also our transcatheter cardiologists who wanted to have another option for the patients of low to intermediate risk, and particularly those that are younger than age 80, for example. And so that developed in January, 2020, and after doing the first one to 200 patients, we’ve opened this up to the rest of the world and we’re very pleased to have a very close collaboration.
Many of the surgeons that are here today, but also all around the world, and there’s now been close to 400 patients that have received this therapy. After commencing this at WVU, so your colleagues and your subscribers that are asking about robotic AVR, there’s been a lot of development overall, the outcomes have been truly outstanding and our key focus is to make this safe, standardized, and reproducible.
And that’s what’s been achieved so far.
Adam Pick: In terms of when you’re using the robot. Is it isolated now just to a robotic AVR procedure? Or has the ability to treat things widened over the years?
Dr. Vinay Badhwar: So that’s a very important question. So there are many options of treating all patients with valvular heart disease.
Transcatheter therapy is a single therapy or a TAVR or TAVI to just treat the aortic valve. But many of our patients that present usually have other things, atrial fibrillation, mitral valve disease, et cetera. Sure we can do isolated aortic valve replacement or repair, uh, done robotically, and that’s definitely a portion. But the whole reason we wanted to develop this through a very right lateral mini thoracotomy incision. That’s a very tiny incision. Is to be able to use the same approach that we use for mitral valve surgery, which is very standardized. We’ve made some small technical modifications, and the whole idea is this.
We strongly feel that this is now a platform not just for isolated aortic valve disease, but for all cardiac surgery, many up to a third of the patients that we do. Are actually concomitant, or in other words, have more than just the aortic valve, a mitral AFib treatment, et cetera. This is a platform for multiple valvular surgery.
Adam Pick: If I’m a patient, getting back to just the robotic AVR, is it for a mechanical valve? Or is it for a tissue valve?
Dr. Vinay Badhwar: Absolutely. So it’s, it’s taking the usual, very standardized surgical treatment. We cut out the valve and sew on a brand new one. This can be either a tissue valve or a biologic valve made of coward pig pig tissue, or a mechanical valve. And there’s been excellent outcomes for both.
Adam Pick: Is there a next step for how you can share this with not just the physicians here, physicians all over the world?
Dr. Vinay Badhwar: Well, thank you for asking. So we’ve, we’ve worked up this in a very transparent way. In fact, innovation in isolation remains in isolation. Innovation as a collaborative. It becomes permanent, at least we hope. And through this, starting in 2022, shortly after initial experiences, we invited surgeons from all around the world to begin to co-develop and share experiences. We’ve now published, uh, last year at the European Association for Cardiothoracic Surgery, the first 300 patients. Which is an international collaboration and multiple sites around the country and the United States as well as Europe. And uh, now this is culminating into over 400 patients and we are hosting another international valve meeting in Morgantown on November 13th and 14th. Uh, it’s called the International VER Symposium, where a surgeon and cardiologist will hopefully share ideas. And their own experiences and how to make this a better therapy for all of our patients.
Adam Pick: Dr. Badwhar, I’ve got two things for you. One is a congratulations on the achievements in robotic AVR, and the second is on behalf of all the patients in our community, all the patients across the world, a big thank you for what you and your team are doing at WVU Heart and Vascular Institute in Morgantown, West Virginia. Thanks for being with me today.
Dr. Vinay Badhwar: It’s a pleasure to be here. Thank you.



