The Reverse Ross Procedure: What Should Patients Know?
Written By: Allison DeMajistre, BSN, RN, CCRN
Medical Expert: Eric Roselli, MD, Chief of Adult Cardiac Surgery, Cleveland Clinic, Cleveland, Ohio
Reviewed By: Adam Pick, Patient Advocate, Author & Website Founder
Published: July 29, 2025
The Ross Procedure is a complex aortic valve replacement operation that offers children and young adults a long-term solution to aortic stenosis and aortic. When the Ross Procedure is successful, patients can have the same quality of life as those without aortic valve disease with no restrictions on activity after recovery. The Ross Procedure involves removing the diseased aortic valve and replacing it with the patient’s own pulmonary valve, called an autograft. A human donor valve, pig valve or cow valve replaces the pulmonary valve.
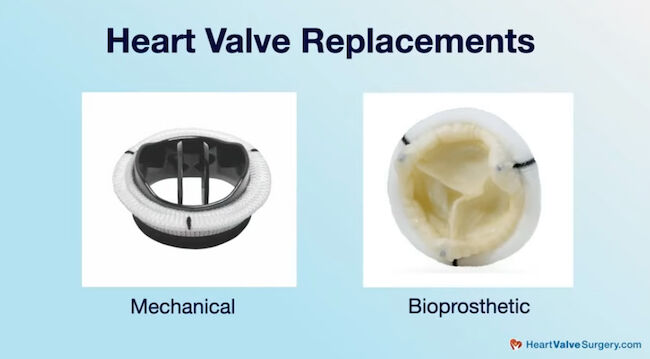
Unlike mechanical valves that are prone to blood clots or biologic valves that may need to be replaced within ten years, the Ross Procedure is less likely to have these complications. Still, there is potential for durability issues with the Ross Procedure due to the high pressure the autograft is under in the aortic position. When a patient’s aortic valve autograft is compromised, one option is to undergo a Reverse Ross Procedure.
Adam Pick, the founder of HeartValveSurgery.com, had a Ross Procedure nearly 20 years ago with no complications, reinterventions, or reoperations, but he had never heard of a “Reverse Ross Procedure” until he saw a patient post about it in the community. He thought it was a great topic to discuss with Dr. Eric Roselli, the Chief of Adult Cardiac Surgery at the Cleveland Clinic in Cleveland, Ohio. Dr. Roselli is a world-renowned heart valve expert who has performed over 3,000 heart valve operations.
Facts About the Reverse Ross Procedure
Here are the key insights shared by Dr. Roselli:
- Valve durability is a priority for younger patients. “When we talk about choosing a biologic aortic valve, it’s all about durability,” said Dr. Roselli. He explained that the Ross Procedure can offer younger patients (typically <50 years) the best chance at durability.
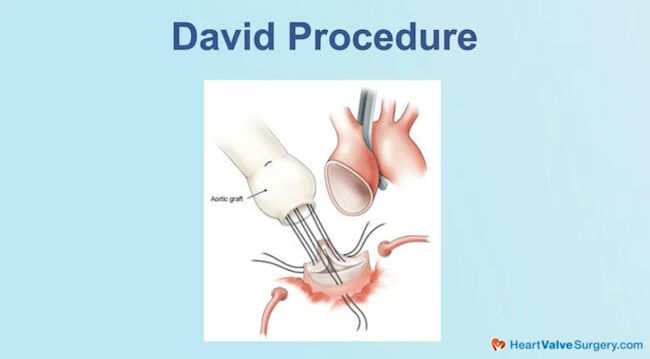
- Saving the patient’s native valve tissue is preferable when possible. “Part of the reason we reinvigorated our adult Ross program was because we were seeing patients come back with late failure of their Ross Procedure,” said Dr. Roselli. “We realized we could do operations where we saved the valve. Sometimes, we turn it into a David’s Procedure if there is an aneurysm around it, and we save the valve if it’s functioning well.
- The Reverse Ross Procedure was pioneered by Dr. Gosta Pettersson. Dr. Roselli stated, “Sometimes, we do an operation pioneered by the great Dr. Gosta Pettersson called the Reverse Ross, which takes the pulmonary valve autograft from the aorta and places it back where it came from. So, you still have your living valve, and we replace the aortic valve with some other choice, either a mechanical or biologic valve.”
- Putting the native valve back to the pulmonary position is an excellent principle of care. “I think it was around 2007 when Dr. Pettersson first started the procedure, and we’ve all learned how to do it,” said Dr. Roselli. “It’s not for every patient, but again, we love this idea of saving the living valve. It’s a great principle of care, and we’ve had experience with over 50 of them. If a patient is the right fit for it, putting the valve back where it came from is a cool choice. Dr. Roselli explained that when the valve isn’t functioning as well in the aortic position, which is a violent environment, but it looks like it is still functional, the autograft can replace the homograft and return to the pulmonary position.
- Pressures in the pulmonary position can be advantageous for the Reverse Ross procedure. Dr. Roselli stated, “Like I always say, the pulmonary valve position is like a lazy river in a resort swimming pool, and the aortic valve is like the Pacific Ocean, a kind of Maverick’s surf environment. So, you can take it and put it back, then replace the aortic valve. It’s a cool way to do a late operation on a Ross, which is a nice option for a patient.”
Thanks Dr. Roselli and the Cleveland Clinic!
On behalf of all the patients in our community, thank you, Dr. Eric Roselli, for everything you and your team are doing at the Cleveland Clinic!
Related links:
- Watch NHL superstar Henrik Lundquist interview his surgeon, Dr. Eric Roselli
- Ask Dr. Eric Roselli: Advanced Surgical Techniques for Aortic Valve Reoperations
- Explore the Cleveland Clinic Heart Valve Microsite
Keep on tickin,
Adam
P.S. For the deaf and hard-of-hearing members of our patient community, we have provided a written transcript of our interview with Dr. Roselli below.
Written by Adam Pick
- Patient & Website Founder

Video Transcript:
Adam Pick: Hi, everybody. It’s Adam with HeartValveSurgery.com. We are in Los Angeles, California at the Society of Thoracic Surgeons Conference. I’m thrilled to be joined by Dr Eric Roselli, who is the Chief of Adult Cardiac Surgery at the Cleveland Clinic in Cleveland, Ohio.
Dr. Roselli., I’m going to call you Eric for the rest of this interview because we’ve known each other for 30 years. Good to see you again.
Dr. Eric Roselli: Yes Adam. Same.
Adam Pick: So verybody knows, we met first at the University of Michigan about 30 years ago. One thing that you and I have talked about over the years is the Ross procedure.
Dr. Eric Roselli: Right.
Adam Pick: Which I went through and had nearly 20 years ago and have had an extraordinary result. No reoperations, no reinterventions.
Dr. Eric Roselli: Awesome.
Adam Pick: I’m not saying that procedure is for everybody with aortic valve disease, but I recently saw something in our community that I’d never seen before, in which a patient posted that they had undergone a reverse Ross procedure with you at the Cleveland Clinic.
And I was hoping you could spend a few minutes with our community sharing what is the reverse Ross operation? How do you use it?
Dr. Eric Roselli: Absolutely. Listen, when we talk about choosing an aortic valve, And we’re choosing a biologic choice. It’s all about durability. And folks want the Ross operation if they’re young and things come together.
Then, because the Ross might offer you the best chance at durability, like the durability you’ve had. Part of the reason we kind of reinvigorated our adult Ross program was because we were seeing patients come back with late failures of their Ross procedure. I don’t know that failure is the right word, degeneration of problems with it, needing another operation, and we realized we could do kind of operations where we still saved the valve.
Sometimes, we turn it into a David’s procedure if there’s an aneurysm around it and we save that valve that’s functioning really well. Then sometimes we do an operation which was really pioneered by the great Dr. Gosta Pettersson from our group, what’s called the reverse Ross, which means he takes that autografted pulmonary valve and we put it back over where it came from.
Which is awesome. So, you still have your living valve. Then, we replace the aortic valve with some other choice, a mechanical or biologic valve. And I think it was around 2007 when Dr. Pettersson first started doing that. And we’ve all learned how to do that. And it’s not for every patient. But again, we love this idea of saving the living valve.
It’s a great sort of principle of care. We’ve had experience with over 50 of these. The operation is done, you know, really well, if you’re a right fit for it, it’s kind of a cool choice to put it back where it came from. And the reason you can do it is if that valve’s not functioning so well anymore in the aortic position, which is a really kind of violent environment for that valve, but still looks like a pretty decent looking, functional, living valve, it can usually do okay in that pulmonary position, where you used to have a homograft, which was dead because that’s a much calmer, low pressure system.
Like I always say, the pulmonary valve position is sort of like a lazy river in a resort swimming pool. And the aortic valve is like the Pacific Ocean, you know, Mavericks surf environment or something like that. So, you can take it and put it back and then you replace the aortic valve and it’s a cool way to sort of do a late operation on a Ross, which is still really nice for a patient, a nice option.
Adam Pick: Well, I love that you are doing everything you can because I’ve always seen you campaign for keeping the living tissue in the heart and going back to what you said at the beginning, it’s all about the durability.
How can you keep that going throughout the patient’s lifetime? Eric, as always, great to see you. Thanks for everything you’re doing at the Cleveland Clinic. Keep it up. And I’m just so happy you could be with us today.
Dr. Eric Roselli: Of course. Thanks Adam.