Ross Procedure: What 4 Questions Should Patients Ask Before Surgery?
Written By: Allison DeMajistre, BSN, RN, CCRN
Medical Expert: Eric Roselli, MD, Chief of Adult Cardiac Surgery, Cleveland Clinic, Cleveland, Ohio
Reviewed By: Adam Pick, Patient Advocate, Author & Website Founder
Published: August 14, 2025
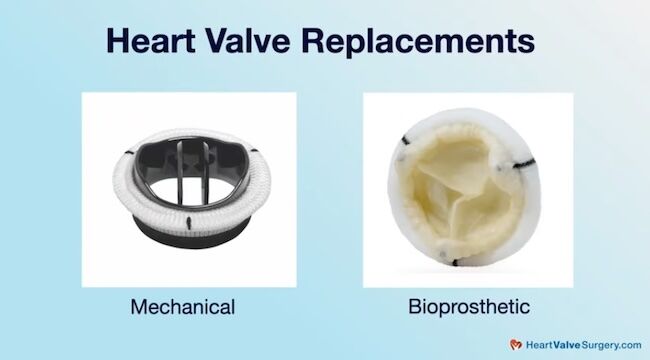
When younger patients with aortic valve disease reach the point they need some type of intervention to repair or replace their valve, one of the most consequential decisions they will make is what kind of surgery to have. A Ross Procedure is an advanced surgical option for younger patients that involves removing the diseased aortic valve and replacing it with the patient’s own pulmonary valve. A donor valve is then implanted in the pulmonary valve’s position. Because of its complexity, patients should understand the intricacies, advantages, and possible limitations before choosing the Ross Procedure.
Adam Pick, founder of HeartValveSurgery.com, is a Ross Procedure recipient. While he’s thankful to be twenty years post-surgery without the need for reoperation, he understands how important it is that patients are mindful of whether the Ross Procedure is right for them. Adam believes one of the best ways to do that is to ask the right questions. Adam recently met with Dr. Eric Roselli, the Chief of Adult Cardiac Surgery at the Cleveland Clinic, and a world-renowned aortic valve expert, to discuss four important questions patients should ask before a Ross Procedure.
What Patients Need to Know About the Ross Procedure
Here are the key insights shared by Dr. Roselli:
- Younger patients and valve choice. Dr. Roselli explained that younger patients need to understand that their goals are part of a shared decision-making process. “I think the first thing a patient should ask is whether they should go with a biologic or mechanical valve, and both are really good. I think that guides the first part of the decision-making. Patients need to know how they feel about anticoagulation and have that discussion with their surgeon. If they want to avoid anticoagulation, that opens a discussion about the biologic choices, which is where the Ross operation fits in.”

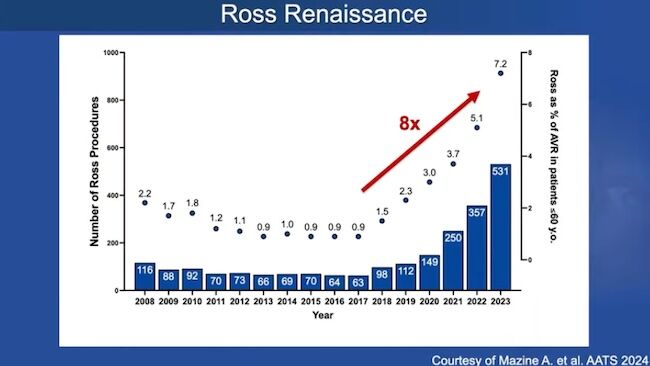
- Patients should consider whether they are a good candidate for a Ross Procedure. Dr. Roselli said, “I know there are a lot of centers building their Ross programs. It’s kind of awesome that we’ve seen a resurgence of it. And Adam, you’re a living example of a wonderful choice made. But I worry a little bit that there may be too much excitement about it because you shouldn’t feel like you’re guaranteed that this living valve choice will absolutely last you a lifetime. That’s concerning to me. In fact, that’s concerning to me when someone chooses a mechanical valve as well, because sometimes you’ll need an operation later in life. When you’re a young patient, we’re looking at decades of survival after your surgery. The way I generally think about a Ross Procedure is it is a great option for younger patients who want to avoid anticoagulation, and maybe it will give them one less operation in their lifetime versus the other biologic choices.”
- Asking about patient outcomes. Given Adam’s experience with the Ross Procedure, Dr. Roselli asked for Adam’s input. “Thanks for flipping the script on me,” said Adam. “If I’m in a meeting with a cardiac surgeon about the Ross, I might ask a question like, ‘What are your outcomes with the patients you’ve treated?’ Dr. Roselli responded, “Absolutely important. During meetings and when I’m speaking to surgeons, there is a slide I use all the time about how the patient is at the core of the decision-making process, but the things we take into account are the disease-specific factors. What are the issues with the valve? Is it regurgitant, bicuspid, etc? What does the aorta look like? Other important health considerations about that patient to ask: Do they have other illnesses? What does their lifelong prognosis look like? Then we have to take into account the surgeon and the center’s experience. What is their experience with providing these various options? I’ll often tell a patient that all the options are on the table, but only because we have great experience and know we can deliver the Ross option really well. Some surgeons may not be comfortable with the Ross, so it may not even be an option. Not because it’s not an option for that patient, it’s just not an option for that patient with that surgical team.”
- Questions about complications. Adam said, “If you’re looking for that center with a specialized ability to do the Ross, I might be concerned with complications. What is your history with complications for the Ross, and how do you manage them? Is that also something that plays around in your algorithm?” Dr. Roselli said, “Yes, 100 percent, and if you know your surgical team isn’t comfortable answering those questions about how many they do and their expected outcomes, at least a ballpark figure, then you might want to ask them if there is someone else you should be talking to.”
Thanks Dr. Roselli and the Cleveland Clinic!
On behalf of all the patients in our community, thank you, Dr. Eric Roselli, for everything you and your team are doing at the Cleveland Clinic in Cleveland, Ohio!
Related Links:
- Cardiac Innovation: The Reverse Ross Procedure with Dr. Eric Roselli
- Explore the Ross Procedure Patient Education Center
Keep on tickin,
Adam
P.S. For the deaf and hard-of-hearing members of our patient community, we have provided a written transcript of our interview with Dr. Roselli below.
Written by Adam Pick
- Patient & Website Founder

Video Transcript:
Adam Pick: Hi, everybody. It’s Adam with HeartValveSurgery.com. We are in Los Angeles, California at the Society of Thoracic Surgeons Conference. I’m thrilled to be joined by Dr Eric Roselli, who is the Chief of Adult Cardiac Surgery at the Cleveland Clinic in Cleveland, Ohio. We are here with Dr. Eric Roselli who I’m going to go ahead and Call Eric.
Dr. Eric Roselli: You must.
Adam Pick: The two of us have known each other for over 30 years. We met all the way back at the University of Michigan. It’s great to see you again, friend.
Dr. Eric Roselli: Good to see you, bro.
Adam Pick: So we’re going talk today about something you and I have been talking about for years-and-years, which is the Ross Procedure operation.
I’ve been thankful to have had one and gone on for nearly 20 years now with no reoperations.
Dr. Eric Roselli: Awesome.
Adam Pick: But patients out there need to be mindful about whether or not this is the right procedure for them and they need to ask some very important questions. So,we’re going to talk about what are the four important questions patients should ask before a Ross procedure.
Maybe we could start, Dr. Roselli, Eric, what would one of them be?
Dr. Eric Roselli: I think the important thing when we’re thinking about valve choice, we’re talking about young patients, okay? We’re talking about valve choice. You need to understand in this shared decision making process what your goals are.
So, I think the first choice a patient should ask themselves is this question about do I go with a biologic choice or a mechanical valve? And both are really good.
I think that guides the first sort of decision making. How do I feel about anticoagulation? And you can have that discussion with your surgeon about it.
If they want to avoid anticoagulation, then that opens a discussion about these biologic choices, which is where the Ross operation fits.
So then another question would be am I a good candidate for that?
I know that there’s a lot of centers are building their Ross programs. It’s kind of awesome that we’ve seen a resurgence of it. Again, you’re a living example of, you know, a wonderful choice made. But, I worry a little bit that there’s maybe too much excitement about it. And the reason is, you shouldn’t feel like you’re guaranteed that this living valve choice is absolutely going to last you a lifetime.
That, that’s concerning to me. In fact, that’s concerning to me when someone chooses a mechanical valve. Because sometimes you need an operation later on in life. And when you’re a young patient, we’re looking at decades of survival after your surgery. The way I generally think about a Ross procedure is it is a great option in younger patients and if you want to avoid anticoagulation, maybe it’s a choice that will give you one less operation in your lifetime versus the other biologic choices.
Lots of good, but you know the questions that we should ask. Why don’t you tell the audience what you think those questions are.
Adam Pick: Thanks for flipping the script on me, Eric. I mean, for me, one of the questions I would think is if I’m at that point where I’m going down the pathway. You described in a meeting with a cardiac surgeon about the Ross, I might ask a question like, “What are your outcomes with the patients that you have treated?”
Dr. Eric Roselli: Absolutely important. You know, at this meeting and one of the meetings, it’s a slide I use all the time when I’m speaking to surgeons, the patient is at the core of that decision making process, but the things we take into account are the disease specific factors. What are the issues with the valve, regurgitant, bicuspid, etc? What does the aorta look like? Other sort of important health considerations about that patient. Like, do you have other illnesses? What does your lifelong prognosis look like? And then, we have to take into account the surgeon and the center’s experience.
What is their experience with providing these various options? So, I’ll tell a patient, hey, for you, all of the choices are on the table, but that’s because we have a great experience and we know we can deliver that Ross option really well. Some surgeons maybe they aren’t comfortable with the Ross, it might not even be an option, but that’s not because it’s not an option for that patient, it’s not, it may just not be an option for that patient with that surgical team.
Adam Pick: Another question, if you’re looking for that center that has the specialized ability to do the Ross, I might be concerned with something like complications. What is your history with complications for the Ross and how do you manage them? Is that something also that plays around in your algorithm?
Dr. Eric Roselli: 100 percent and if you know your surgical name isn’t comfortable asking answering those questions about how many they do, what they expect the outcomes to be like, at least a ballpark figure of those things and you’re interested in it, then you might want to ask them if there’s someone else you should be talking to.
Adam Pick: Eric, this has been really different. You and me coming together on brainstorming questions for patients, and I’ve had a lot of fun as always being your friend and also being your colleague here as we educate these patients about the Ross procedure and on behalf of the patients Thanks to you and your team for everything that you are doing at the Cleveland Clinic.
Dr. Eric Roselli: Thanks to you and your team for educating everybody. It’s awesome. Thank you.




