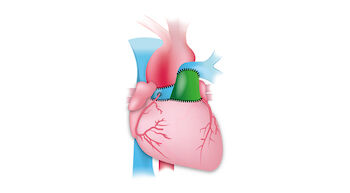
The Ross Procedure: An Advanced Type of Aortic Valve Replacement
The Ross Procedure helps aortic valve patients achieve normal life expectancy without the use of blood thinners.1
The Ross Procedure: An Advanced Type of Aortic Valve Replacement
The Ross Procedure helps aortic valve patients achieve normal life expectancy without the use of blood thinners.1
“For the right patient, the Ross Procedure provides favorable long-term outcomes and excellent quality-of-life.”
-- Dr. Vaughn Starnes, Surgeon-in-Chief at
Keck Medicine of USC, Los Angeles, California
-- Dr. Vaughn Starnes, Surgeon-in-Chief at Keck Medicine of USC, Los Angeles, California.
Learn important facts about the Ross Procedure in this video with Dr. Vaughn Starnes, a world-renowned Ross Procedure surgeon, who has performed over 650 Ross Procedures.
"I did A LOT of research on my valve replacement options. The Ross Procedure provided me a normal quality-of-life without blood thinners."
-- Andy Dial, Ross Procedure patient of Dr. Christopher Burke
-- Andy Dial, Ross Procedure patient Dr. Christopher Burke
Each year, over 500 Ross Procedures are performed in the United States2 on aortic valve patients that are typically active, have more than 20 years of life expectancy and do not want to be on blood thinners. Watch this video with Andy Dial, a Ross Procedure patient to learn about his experience.
4 Questions to Ask Your Surgeon Before a Ross Procedure
The Ross Procedure is very complex and requires a high level of surgical precision and skill. Learn the four must-ask questions of your potential Ross Procedure surgeon in this video with Dr. Eric Roselli, the Chief of Adult Cardiac Surgery at Cleveland Clinic in Cleveland, Ohio.
Find Experienced Ross Procedure Surgeons
The Ross Procedure is a specialized form of aortic valve replacement that is only performed at select cardiac centers that have dedicated teams for this unique heart valve therapy.
“New research shows normal life expectancy is acheived from the Ross Procedure even if a reoperation is needed.”
-- Dr. William Brinkman, Director of the Aorta Program at
Baylor Scott & White The Heart Hospital in Plano, Texas
-- Dr. William Brinkman, Director of the Aorta Program at Baylor Scott & White The Heart Hospital in Plano, Texas
At the recent Society of Thoracic Surgeons Conference, Dr. William Brinkman shared new research that the Ross Procedure helps aortic valve patients obtain normal life expectancy even if a reoperation is needed. Watch this video to learn more.
Do I Need To Get on a "Waiting List" to Receive a Human Donor Valve During the Ross Procedure?
During the Ross Procedure, a human donor valve is typically used to replace the patient’s pulmonary valve. Watch this video with Dr. Joanna Chikwe, the Chair of Cardiac Surgery at Cedars-Sinai Medical Center in Los Angeles, California, to learn if patients need to get on a waiting list to undergo the Ross Procedure.
Can Aortic Valve Patients With an Aortic Aneurysm Get the Ross Procedure?
According to research, approximately 50% of patients with bicuspid aortic valve disease are also diagnosed with a thoracic aortic aneurysm (a bulging of the aorta).3 Watch this video with Dr. Chris Malaisrie, Co-Director, Heart Valve Center at Northwestern Medicine in Chicago, Illinois, to learn if patients with aortic aneurysms can undergo the Ross Procedure.
Can The Ross Procedure Be Used for Children With Aortic Valve Disease?
Treating children with aortic valve disease is very challenging. Watch this video with Dr. Vaughn Starnes, Surgeon-in-Chief at Keck Medicine of USC in Los Angeles, California, to learn how he uses the Ross Procedure to help younger patients.
Free Patient eBook
To learn more about the Ross Procedure, click here to download our new Free eBook, “The Ross Procedure: What 8 Facts Should You Know?” You can share this eBook with your family and friends.
Top 8 Patient Questions About The Ross Procedure
Question 1: How do I know if I am a good candidate for the Ross Procedure?
It is important for patients with aortic valve disease to understand that the Ross Procedure is not for every patient. Watch this video with Dr. Craig Baker, the Chief of Cardiac Surgery at Keck Medicine of USC in Los Angeles, California, to learn if the Ross Procedure may be for you given your specific anatomy, your lifestyle, and your health goals.
Question 2: How might wrapping the pulmonary autograft in Dacron enhance the durability of the Ross Procedure?
An innovation for the Ross Procedure has been the use of Dacron to support the pulmonary autograft. In this video, Dr. Christopher Burke, Co-Director of the Multi-Disciplinary Thoracic Aorta Program at UW Medicine Heart Instititue in Seattle, Washington, explains why and how this technique may lead to better durability for Ross Procedure patients.
Question 3: How might patients evaluate mechanical valves, biological valves and the Ross Procedure?
Learn key differences between mechanical heart valves, biological valves, and the Ross Procedure in this video with Dr. Craig Baker, Chief of Cardiac Surgery at Keck Medicine of USC.
Question 4: How and why do surgeons inspect the pulmonary valve during a Ross Procedure?
In a Ross Procedure, the patient's pulmonary valve is used in place of the diseased aortic valve. How do surgeons know if the pulmonary valve is a good candidate to use? Get the answer from Dr. William Brinkman, Director of the Aorta Program at Baylor Scott & White The Heart Hospital in Plano, Texas, in this video.
Question 5: What is the reverse Ross Procedure? How is it used to help patients?
To save the patient’s own valvular tissue if a Ross Procedure requires a reoperation, there is a new cardiac innovation known as the “Reverse Ross Procedure”. Learn more in this video with Dr. Eric Roselli, the Chief of Adult Cardiac Surgery at Cleveland Clinic in Cleveland, Ohio.
Question 6: How should patients go about finding a Ross Procedure surgeon?
Finding a surgeon that specializes in the Ross Procedure can be difficult. In this video, Dr. Richard Kim, the Director of Pediatric and Congenital Cardiac Surgery at Cedars-Sinai Medical Center in Los Angeles, California, shares key insights for patients considering the Ross Procedure.
Question 7: How is the North American Ross Consortium helping patients get excellent outcomes?
The North American Ross Consortium was founded to study the technical aspects of the Ross Procedure and attempt to understand anatomical issues that effect outcomes. Learn more from Dr. William Brinkman, Director of the Aorta Program at Baylor Scott & White The Heart Hospital in Plano, Texas, in this video.
Question 8: How are Ross Procedure Centers evolving to help patients with aortic valve disease?
Given the complexity of the Ross Procedure, medical teams need to develop, resource and staff unique competencies to successfully compete the Ross Procedure. Watch this video to learn how Dr. Christopher Burke, Co-Director, Multi-Disciplinary Thoracic Aorta Program, and his team at UW Medicine Heart Institute in Seattle, Washington have evolved their cardiac center to meet the growing patient demand for the Ross Procedure.
References
- Dr. William Brinkman, et al., “Outcomes of Redo Operations After Ross Procedure”, a presentation at The Society of Thoracic Surgeons Meeting, January, 2024.
- Dr. Amine Mazine, “The Ross Resurgence: North American Trends in Utilization and In-Hospital Outcomes”, American Association for Thoracic Surgey, April, 2024.
- Jasjit Rooprai, BSc, et al., “Thoracic Aortic Aneurysm Growth in Bicuspid Aortic Valve Patients: Role of Aortic Stiffness and Pulsatile Hemodynamics”, Journal of the American Heart Association, April, 2019